Non-traumatic injuries are usually caused by overuse, which may or may not be accompanied by improper technique. We are talking about chronic injuries.
To reach the correct diagnosis and thus apply the appropriate treatment, as with all injuries in any athlete, a complete medical history with a detailed anamnesis is necessary, asking where the greatest pain point or injury is, how the pain or injury appeared, how long it has been present, its evolution since the pain or injury began, if there is any situation that improves or worsens it,... But also, in the case of injuries in cyclists or triathletes, it will be very helpful to evaluate the athlete on the bike, thus exploring their position and proper adaptation to the bike. Very frequently, these non-traumatic injuries occur due to a poor or incorrect adaptation to the bike.

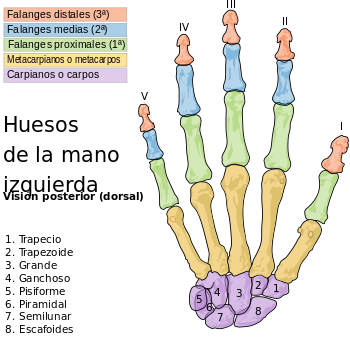
Anatomical review of the upper limb
The hand has three areas with 27 bones in total: carpus (wrist with 8 bones), metacarpus (with 5 bones) and fingers. The forearm has 2 bones (ulna and radius) and the arm has only 1, the humerus.
The anatomical description of muscles, tendons, ligaments, arteries, veins and nerves is quite complex, so we will not delve deeper than what the images can provide.
Cycling injuries
People who practice cycling (cyclists and triathletes) frequently present with upper limb injuries very different from those in other sports where injuries such as epicondylitis, rotator cuff tendinopathy or others predominate. In this sport, other injuries appear, which are described below:

Carpal Tunnel Syndrome:
It appears as a consequence of median nerve compression. It can even appear as a consequence of small microtraumas at the same level with peripheral inflammation and nerve irritation. Likewise, if the hand is placed on the upper part of the handlebars, with the carpus in maximum extension, excessive elongation of the nerve will occur, also causing irritation.
As a consequence, the symptomatology that appears is an alteration of fine motor activity, hypoesthesia and paresthesia (numb fingers) of the thumb, index, middle and half of the ring finger. This situation is described by patients as "butter fingers" as they often drop objects due to lack of grip strength. In the examination, we usually find a positive Phalen's maneuver (maintaining maximum wrist flexion for one minute) and an equally positive Tinel's sign (paresthesias are reproduced with percussion over the compressed area).
This symptomatology usually only occurs with sports practice and disappears outside the sporting environment.
As a treatment, the first option will be to perform a detailed biomechanical study, with the pertinent modifications at different levels, saddle, handlebars, handlebar stem,... This is usually the only treatment since the symptomatology usually disappears with the pertinent corrections, but if the symptomatology persists, ultrasounds, X-rays, and even MRIs would have to be performed to resolve the situation.
2. Guyon's Canal Syndrome:
In this case, the affected nerve is the motor branch of the ulnar nerve. The mechanism is usually the same as in Carpal Tunnel Syndrome, microtrauma or continuous compression at the Guyon's Canal level with nerve irritation. This compression of the ulnar nerve occurs when the hand is positioned on the upper part of the handlebars with maximum carpal extension. The symptomatology that appears is also hypoesthesia and paresthesias, even with loss of strength in the fifth and fourth fingers. Watemberg's sign (permanent separation of the 5th finger) and Frament's sign (hypothenar atrophy and ulnar claw of the last two fingers) usually appear.

3. De Quervain's Tenosynovitis
De Quervain's tenosynovitis is the inflammation of the abductor pollicis longus and extensor pollicis brevis, at the level of the radial styloid process. It usually arises as a consequence of resting the wrist on the handlebars with ulnar deviation. This alteration of the position at the handlebar level causes an angulation of the aforementioned tendons. What actually occurs is an inflammation at the level of the fibrous-osseous tunnel, which is called tenosynovitis.
Intense pain appears at the level of the radial styloid. The pain worsens with Finkelstein's maneuver, which is positive in this case.

4. Tenosynovitis of the radial extensors and finger extensors.
This injury arises in cyclists or triathletes who train or compete long distance and whose road surface is uneven, cobbled or paved. When training on this type of surface, the athlete grips the handlebars more firmly, as a result, the forearm muscles are overloaded, producing hypertrophy of the abductor pollicis longus and extensor pollicis brevis muscles, which run over the radial extensors, which are compressed against the deep planes.
Continuous pain usually occurs with wrist flexion-extension movements, and sometimes a slight crepitation is heard. When the injury becomes chronic, an inflamed area sometimes appears on the dorsal side of the radius due to chronic inflammation of the radial extensors. The forearm muscles are overloaded, producing hypertrophy of the abductor pollicis longus and extensor pollicis brevis.
Treatment
Sometimes, it is necessary to perform some diagnostic imaging test to assess the degree of the injury. Ultrasound, or nuclear magnetic resonance (NMR) are usually the techniques of choice.
In this type of injury, the best treatment will be prevention. There is no doubt that a biomechanical study where our anthropometric measurements are adjusted to the bike will be the best measure we can take. It is even advisable that we could do this study before buying a bike to choose not only by colors, brand or design, but also by being the brand and model that best suits our anthropometry. In some cases, it will be necessary to change the training routes with another type of asphalt, more regular. If you want to know more about biomechanics in cycling, click here.
Once the pertinent changes have been made to the bike, there will be an adaptation phase until we feel comfortable. In addition, with this type of study, we will achieve a more efficient pedal stroke.
On the other hand, if the injury appears from the point of view of conventional medicine, the much-questioned NSAIDs (non-steroidal anti-inflammatory drugs) and even corticosteroid infiltrations will be used. There is some consensus document from specialists in sports medicine that indicates that the use of NSAIDs can chronicize sports injuries.
Going to the physical therapist early will ensure a quick recovery by using techniques such as ultrasound, Cyriax massage, dry needling, kinesiotaping,... In recent years, Diathermy (radiofrequency) has positioned itself as the treatment of choice along with the physical therapist's manual work. All these techniques and others are used at Sportsalud, for the early recovery of our athletes.
As an alternative to NSAIDs, we can use supplements of B vitamins and also Magnesium, as these reduce nerve irritation and also act as muscle relaxants. In addition, we can use natural anti-inflammatory supplements such as Turmeric (for example Green Flex). The use of an anti-inflammatory cream based on CBD together with other active components such as arnica (CBD-Cream) will help a faster recovery. We should not forget high-quality collagen-based supplements such as the internationally recognized Peptan (Collagen Plus), which we can use as a preventive or as a treatment, since collagen peptides are precursors of structural proteins such as collagen itself, or elastin,... glycoproteins that are essential in different tissues (tendons, ligaments, joints,...).
In conclusion, for pain in sports and also as a recommendation, you should always go to a doctor for proper assessment and treatment. Injuries start small and gradually increase because we don't always stop training. Professional athletes always go to their primary doctor or physical therapist to recover as soon as possible.

Dr. Sacristán
Compartir:
Does creatine monohydrate increase muscle mass?
How to harness the benefits of plant-based proteins in sports